Connecting Patients, Research & Intelligence for Better Outcomes
One integrated ecosystem that turns biological complexity into precision therapeutic decisions.
AiM One Health connects patients and communities, an open clinical & scientific network, and a governed AI core platform into one explainable, fully traceable system — turning consented data, multi-omics, and live evidence into precision decisions for the diseases that need them most: rare disease, oncology, and immune disorders. Better outcomes, accelerated research, real-world impact.
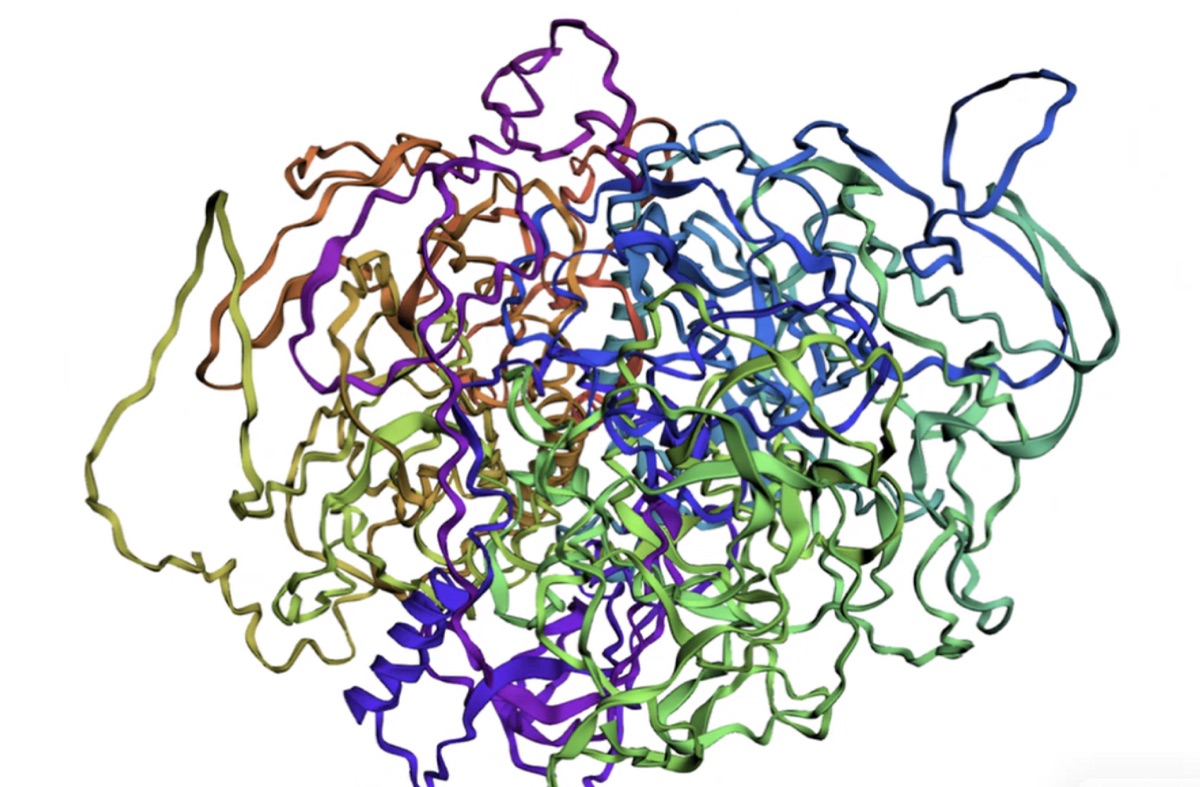
nexmif_esmfold.pdb
11,734 atoms
Style
Cartoon
Stick
Sphere
Surface
Line
Step 7 of 8
all 4 subagents done
ESMFold · pLDDT ready
AI Discovery
Multidisciplinary
Evidence Intel
Virtual Cell
Gene Fold
Translational
Explainable AI
Governance
Traceability